 Rehabilitáció csak online elérhető
Rehabilitáció csak online elérhető
 E-mail: paleomedicina@gmail.com
E-mail: paleomedicina@gmail.com


Zsófia Clemens, Andrea Dabóczi, Csaba Tóth
INTRODUCTION: Outlook for cancer patients remains poor despite ”best available treatment” which includes surgery, chemotherapy and radiotherapy in most solid cancers. Genetic profiling attempts to use matched chemotherapy and the use of high-cost biological therapies, so far, did result in no major breakthrough (1). Metabolic therapies have been suggested as a promising alternative option. Yet, clinical group studies that have been published, provide next to no evidence for a benefit in hard clinical endpoints of cancer. Previously, we put forward (2) that the apparent ineffectivity of the ketogenic diet in cancer is likely due to two factors. First, all published studies included cancer patients that also used chemo- and/or radiation therapy. Second, all group studies used the classical version of the ketogenic diet which is based on vegetable oils and dairy, an evolutionary maladapted, erroneous version of the ketogenic diet.
METHOD: Since 2011 we have been using the paleolithic ketogenic diet (PKD) in the treatment of chronic diseases including cancer. The PKD is an animal meat-fat-based diet similar to that originally proposed by Voegtlin in 1975 (3). In our database, there are 70 cancer patients who meet the criteria of following the PKD for at least two months. Out of these patients, we present two cases where the disease first recurred after the standard oncological treatment. Later on, both patients stopped standard oncotherapy, and decided to use PKD as a stand-alone therapy. The two patients were in a close follow-up and experienced stable disease and regression, respectively. In addition, out of our database, we have selected the best-performing patients (having a follow-up of and being progression-free for 2< years, and being alive at the time of the current analysis). It was our aim to find out what they have in common.
PATIENT #1
Cancer type: Recurrent glioblastoma (grade 4 brain cancer)
Age: 53 years old (at diagnosis)
Medical history: bladder cancer, high blood pressure
Therapy 1 (Jan – May 2016: 4 months):
Surgery+chemotherapy+radiotherapy → Aug 2016 recurrence
Therapy 2 (Sep 2016 – currently: 30 months):
PKD alone → progression-free, symptom-free, medicine-free
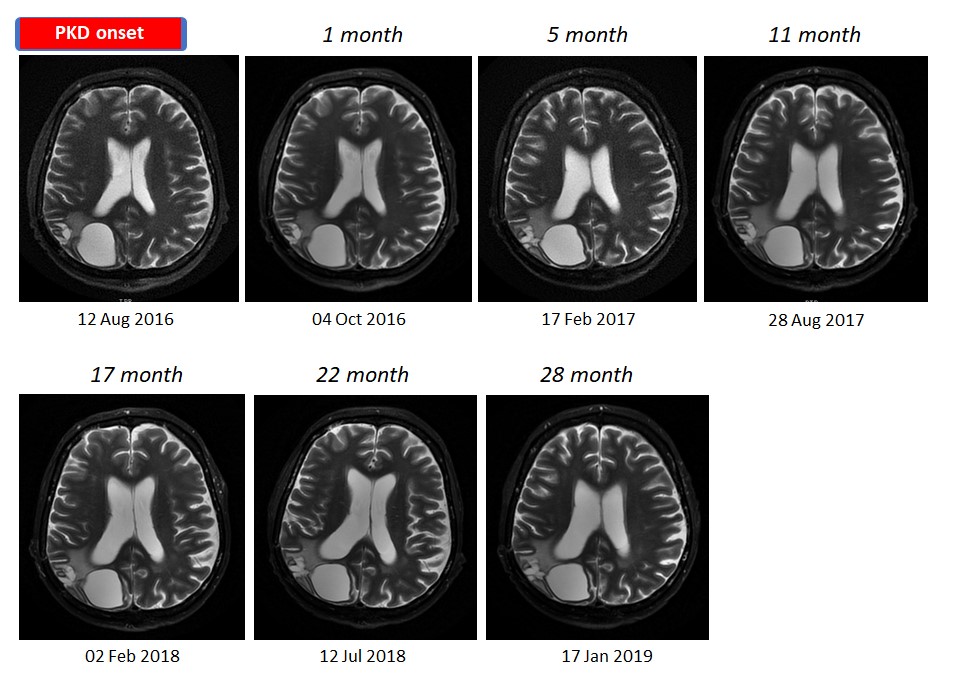
Follow-up MRI scans
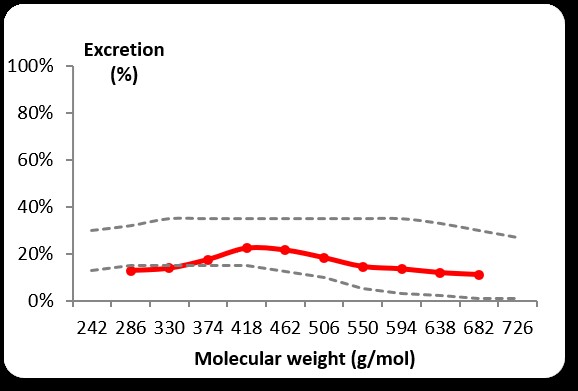
Intestinal permeability measurement (PEG400): normal at 17 months on the PKD.
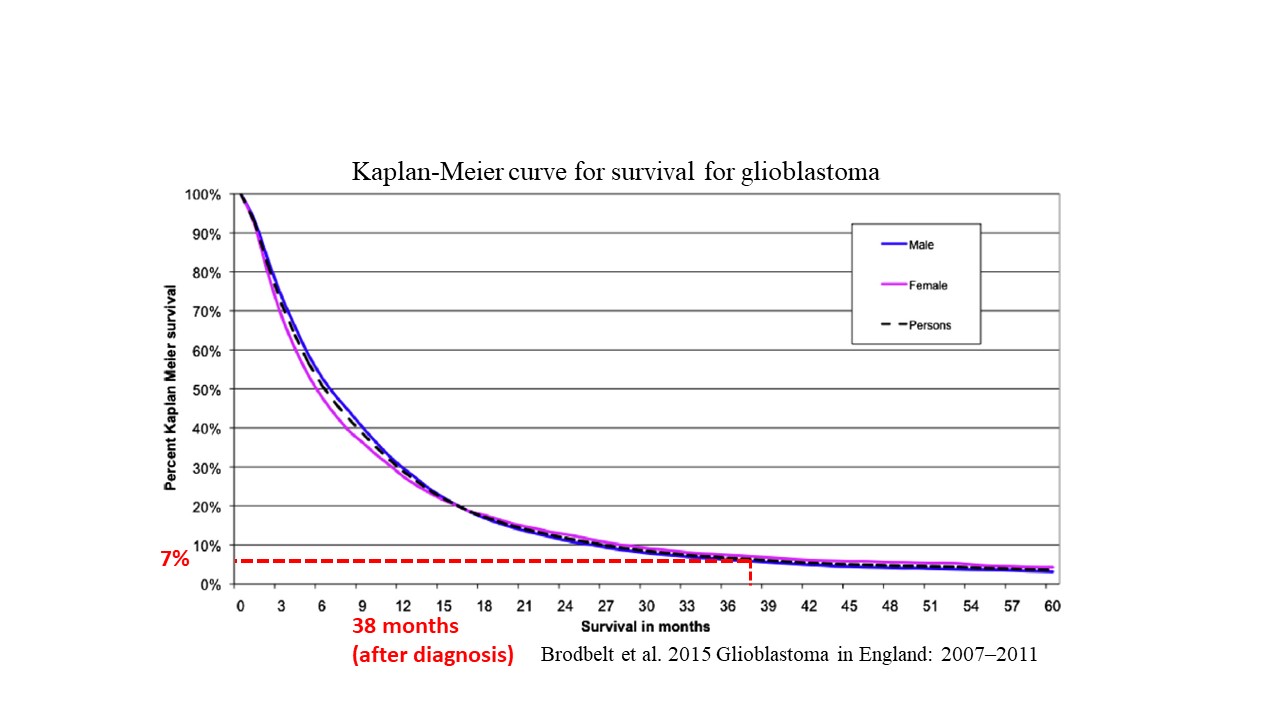
Kaplan-Meier curve for glioblastoma survival for 10,743 patients from the National Cancer Registration Service (UK) vs. Pat#1 survival
PATIENT #2
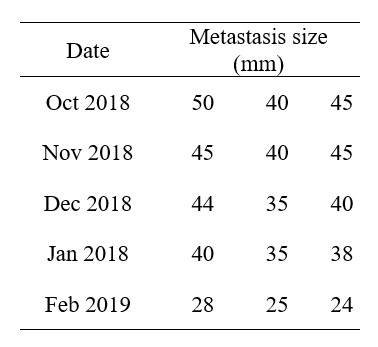
Cancer type: recurrent cancer (metastasis of breast cancer in new locations: in the liver and in the hip bone)
Age: 46 years old (at recurrence)
Medical history: invasive ductal carcinoma of the breast (2013)
Therapy 1: surgery, chemotherapy, radiotherapy, hormone therapy (2013 – 2018) → metastasis (liver, hip bone)
Therapy 2: PKD alone (Oct 2018 – currently: 5 months) → regression in the size and metabolic activity of the metastases
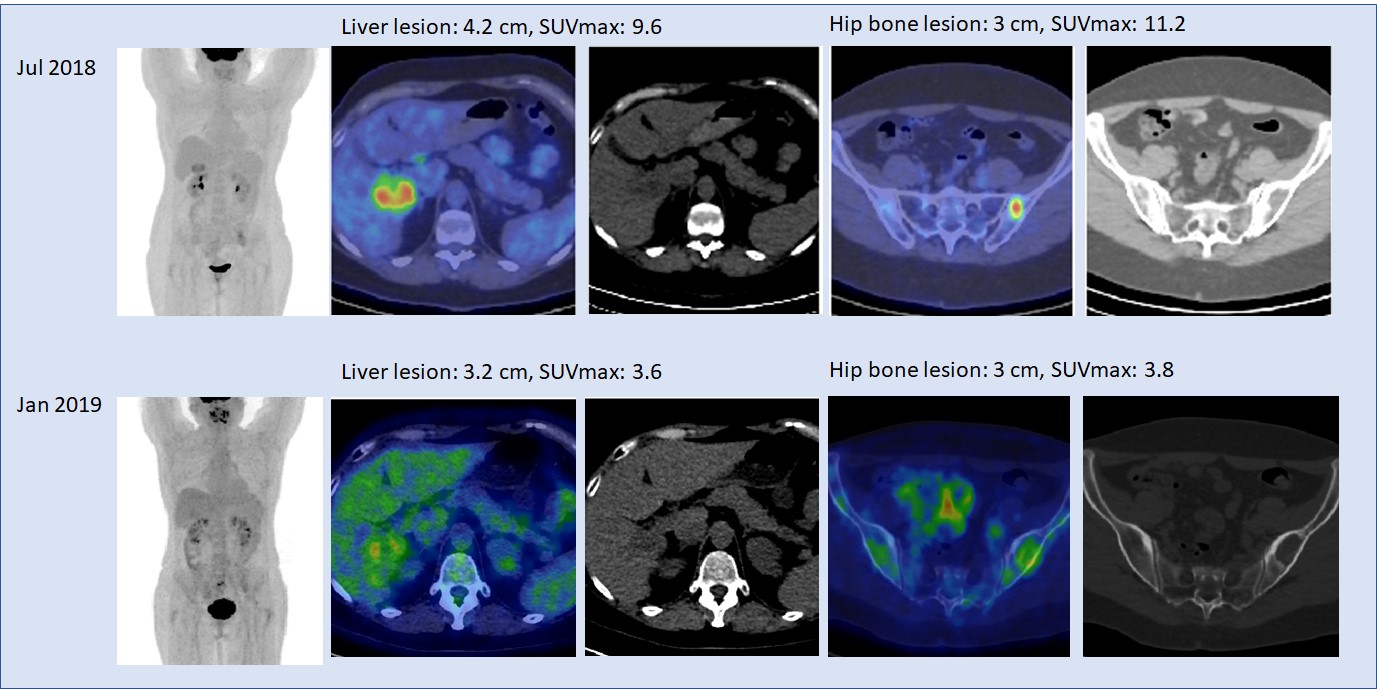
PET-CT
Ultrasound of the liver
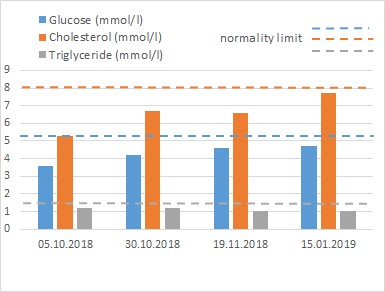
Blood work
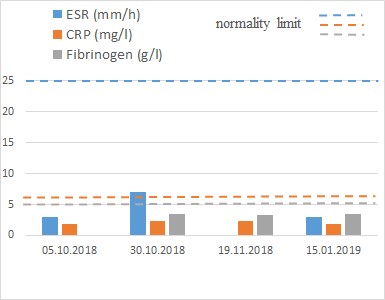
Blood work
PATIENTS #3,4,5,6,7
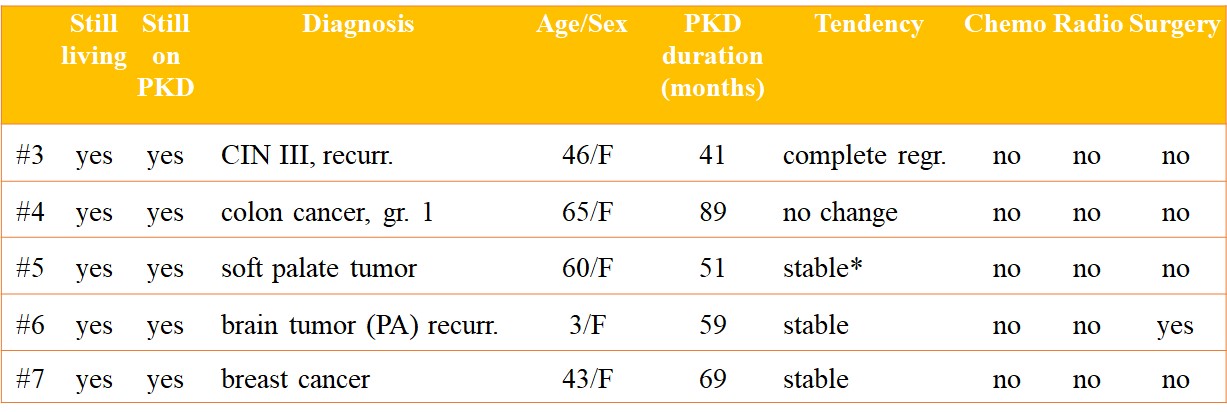
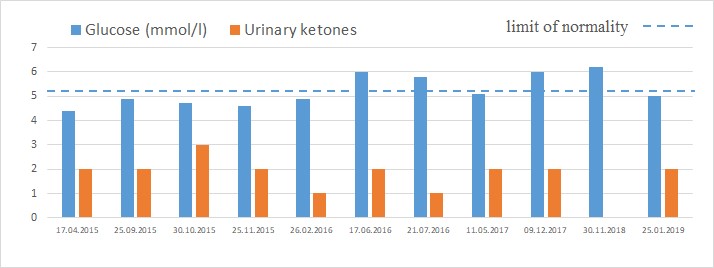
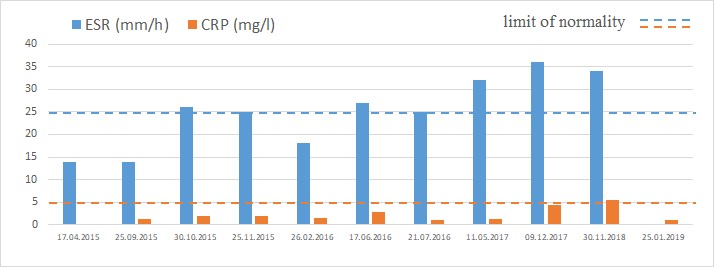
* Stable for 25 months, then slight progression with decreasing adherence (see graphs for blood glucose, urinary ketones, ESR and CRP)
* PATIENT #5

CONCLUSIONS: Pat#1 with recurrent glioblastoma showed stable tumor size for the last 30 months. Pat#2 with recurrent metastasis showed a significant decrease in the size and the metabolic activity of the metastasis in five months. Both patients used the PKD as a stand-alone therapy. Retrospective analysis showed that our best performing cancer patients strictly adhered to the diet and received no chemotherapy or radiotherapy. These patients were also not taking supplements or medicines. By contrast, out of the 70 patients in our database, no patient receiving chemotherapy or radiotherapy was progression-free at two years (even with strict PKD adherence). Chemo- and/or radiation therapy possibly decreasing efficacy of metabolic therapies was previously also suggested by Seyfried et al (4).
REFERENCES
1. Aggarwal A, Fojo T, Chamberlain C, et al. Do patient access schemes for high-cost cancer drugs deliver value to society?-lessons from the NHS Cancer Drugs Fund. Ann Oncol. 2017 Apr 27.
2. Csaba Tóth, Andrea Dabóczi, Madhvi Chanrai, et al. Comment on “Systematic Review: Isocaloric Ketogenic Dietary Regimes for Cancer Patients” by Erickson et al. Journal of Cancer Research and Treatment. Vol. 5, No. 3, 2017, pp 86-88.
3. Voegtlin WL. The stone age diet: based on in-depth studies of human ecology and the diet of man. New York: Vantage Press, 1975.
4. Seyfried TN, Shelton LM, Mukherjee P. Does the existing standard of care increase glioblastoma energy metabolism? Lancet Oncol. 2010;11:811–3.
Zsófia Clemens, Andrea Dabóczi, Csaba Tóth
ICMNI – Paleomedicina Hungary
Low Carb Denver Conference, 2019
2019-03-16